Printable Blank Hcfa 1500 Form
2012 2020 Form Cms 1500 Fill Online Printable Fillable
Cms 1500 Template

Hcfa Form Fill Online Printable Fillable Blank Pdffiller

7500 security boulevard baltimore md 21244.
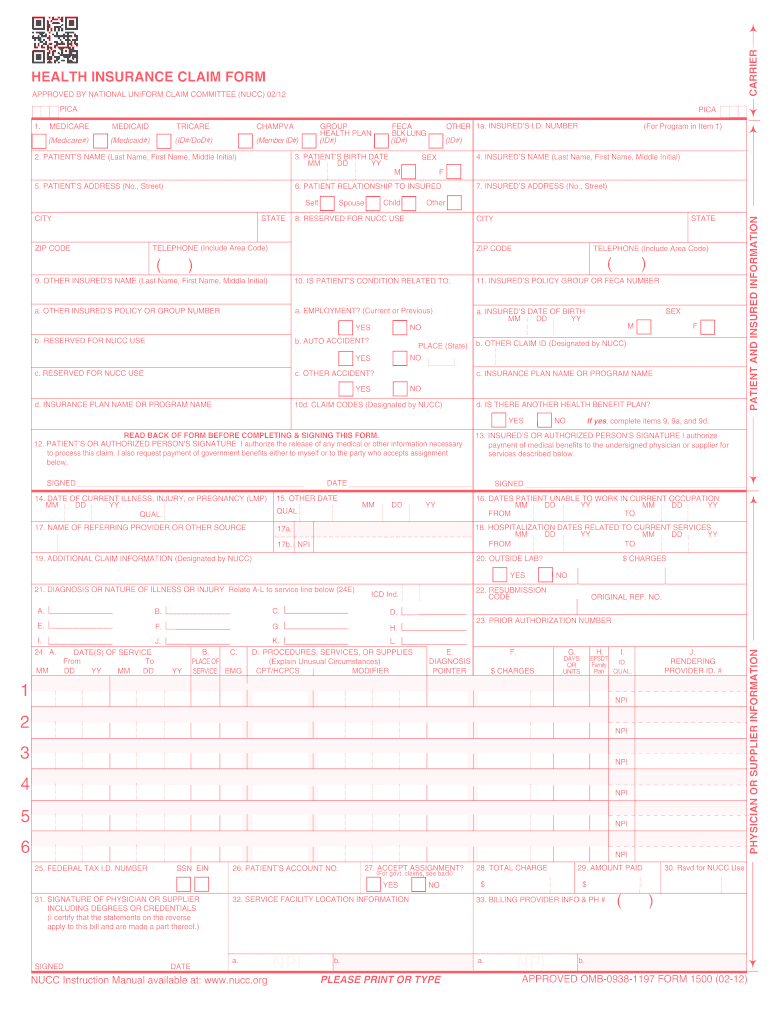
Printable blank hcfa 1500 form. Download cms claim form 1500 which is used by health care professionals to bill medicare and medicaid. Download the fillable hcfa 1500 claim form that is both a fillable andor printable medical claim form that will provide insurance illness and injury information for medical services claimsif the user would like to complete the form online simply download click inside the box to begin and begin typing your information. Patient information blocks 2 8. In essence it is a claims form that the medical professional or the medical office completes and submits to the health insurance company.
Otherwise here is an abridged version of instructions to fill out the hcfa 1500 claim form. How to submit claims. Required fields on the form are marked required. Claims must be made within 12 months after services are provided.
Please print or type approved omb 0938 0008 form cms 1500 12 90 form rrb 1500 approved omb 1215 0055 form owcp 1500 approved omb 0720 0001 champus because this form is used by various government and private health programs see separate instructions issued by. An hcfa 1500 form is used to document a medical procedure. In addition to medicare parts ab and for medicare durable medical equipment administrative contractors. Free hcfacms 1500 form template for medical claims in fillable format.
Claims may be electronically submitted to a medicare carrier durable medical equipment medicare administrative contractor dmemac or ab mac from a providers office using a computer with software that meets electronic filing requirements as established by the hipaa claim standard and by meeting cms requirements contained in the provider enrollment certification. Cms 1500 pdf home a federal government website managed and paid for by the us. Blank cms 1500 forms these blank cms 1500 forms are fully updated with the 0212 latest revisions 100 compliant and printed to exact specifications for layout paper and ink. The cms 1500 form is the standard paper claim form used by a non institutional provider or supplier to bill medicare carriers and medicare administrative contractors macs when a provider qualifies for a waiver from the administrative simplification compliance act asca requirement for electronic submission of claims.
Required box 2 last name first name middle initial if any box 3 date of birth and sex. The cms hcfa 1500 form is the standard paper claim form used by a non institutional provider or supplier to bill medicare carriers and medicare administrative contractors macs when a provider qualifies for a waiver from the administrative simplification compliance act asca requirement for electronic submission of claims.
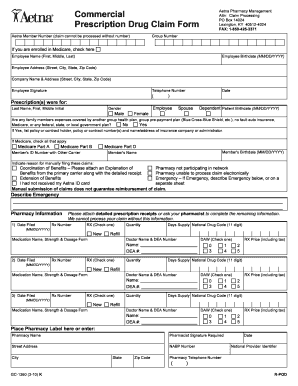
Aetna Hcfa 1500 Form Fill Online Printable Fillable
Hcfa Cms 1500 Medicare Insurance Claim Form Software

Just Cms 1500 Forms New Blank Cms 1500 Hcfa Form Version

Cms 1500 Free Download Form

2012 2020 Form Cms 1500 Fill Online Printable Fillable

Cms 1500 Free Download Create Edit Fill And Print Pdf

1500 Claim Form Free New New Cms 1500 Claim Forms Hcfa

Blank Cms 1500 Form

Cms 1500 Form Template Download Free
Blank Cms 1500 Form Pdf Download Form Resume Examples

New Cms 1500 02 12 Claim Form 25 Forms
Hcfa 1500 Sample Fill Online Printable Fillable Blank

Cms 1500 Claim Forms Hcfa Version 02 12 1 Part Laser Pkg Of 500

Cms 1500 Blank Paper Claim Form Student Health Insurance

Free Fillable Cms 1500 Template And Information Blue

Tmppm 2008 5 5 3 Cms 1500 Blank Claim Form

Free Cms 1500 Form New Medical Claim Form 1500 Templates
Medical Billing Process Cms 1500 Claim Form Billing Instruction
